
The Patient section for a dental claim is used to supply the patient information. This information is required when the patient is the subscriber or considered to be the subscriber and at least one of the element requirements is met.
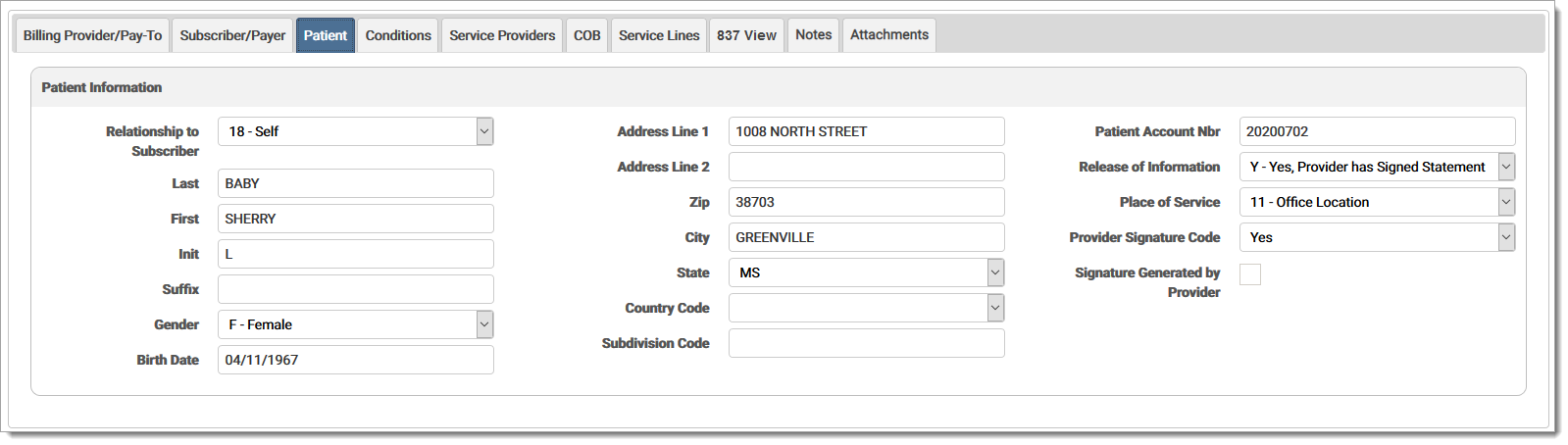
The Patient fields are defined below:
Relationship to SubscriberRelationship to Subscriber
Code indicating the relationship of the patient to the person insured. Required when the patient is the subscriber or is considered to be the subscriber. Options are:
| 01 | Spouse |
| 18 | Self |
| 19 | Child |
| 20 | Employee |
| 21 | Unknown |
| 39 | Organ Donor |
| 40 | Cadaver Donor |
| 53 | Life Partner |
| G8 | Other Relationship |
Last name of the person to whom the services were provided.
First name of the person to whom the services were provided.
Middle initial of the patient.
Additional descriptive information at the end of the patient's name (e.g. Jr.).
The gender of the patient as recorded at date of admission, outpatient service, or start of care. Options are:
|
F |
Female |
| M | Male |
| U | Unknown |
The date of birth of the patient.
Street number and name of the mailing address of the patient (or post office box number or RFD), and additional address information.
Postal code of the address where the patient lives. When a user enters a zip code in a zip code field and clicks tab to move to the next field, the city and state fields are automatically generated based on data received from the USPS. Note: This replaces any data already entered in the city/state fields.
Name of the city where the patient lives.
Two-letter code for the state or province where the patient lives.
The country where the patient lives.
Subdivision CodeSubdivision Code
Code identifying the country subdivision.
Patient Account NumberPatient Account Number
Patient’s unique alpha-numeric number assigned by the provider to facilitate retrieval of individual financial records and posting of the payment.
Release of Information CodeRelease of Information Code
Code indicating whether the provider has on file a signed statement permitting the release of medical data to other organizations.
| I | Informed Consent to Release Info |
| Y | Yes, Provider has Signed Statement |
Place of ServicePlace of Service
Code identifying the type of facility where services were performed. The drop-down menu displays the options. Options are:
| 01 | Pharmacy |
| 02 | Telehealth |
| 03 | School |
| 04 | Homeless Shelter |
| 05 | Indian Health Service Free-Standing Facility |
| 06 | Indian Health Service Provider-Based Facility |
| 07 | Tribal 638 Free-Standing Facility |
| 08 | Tribal 638 Provider-Based Facility |
| 09 | Prison/Correctional Facility |
| 10 | Unassigned |
| 11 | Office Location |
| 12 | Home |
| 13 | Assisted Living Facility |
| 14 | Group Home |
| 15 | Mobile Unit |
| 16 | Temporary Lodging |
| 17 | Walk-In Retail Health Clinic |
| 18 | Place of Employment/Worksite |
| 19 | Off Campus Outpatient Hospital |
| 20 | Urgent Care |
| 21 | Inpatient Hospital |
| 22 | On-Campus Outpatient Hospital |
| 23 | Emergency Room Hospital |
| 24 | Ambulatory Surgical Center |
| 25 | Birthing Center |
| 26 | Military Treatment Facility |
| 31 | Skilled Nursing Facility |
| 32 | Nursing Facility |
| 33 | Custodial Care Facility |
| 34 | Hospice |
| 41 | Ambulance - Land |
| 42 | Ambulance - Air or Water |
| 49 | Independent Clinic |
| 50 | Federally Qualified Health Center |
| 51 | Inpatient Psychiatric Facility |
| 52 | Psychiatric Facility - Partial Hospitalization |
| 53 | Community Mental Health Center |
| 54 | Intermediate Care Facility/Individual with Intellectual Disabilities |
| 55 | Residential Substance Abuse Treatment Facility |
| 56 | Psychiatric Residential Treatment Center |
| 57 | Non-Residential Substance Abuse Treatment Facility |
| 60 | Mass Immunization Center |
| 61 | Comprehensive Inpatient Rehabilitation Facility |
| 62 | Comprehensive Outpatient Rehabilitation Facility |
| 65 | End-Stage Renal Disease Treatment Facility |
| 71 | Public Health Clinic |
| 72 | Independent Laboratory |
| 82-98 | Unassigned |
| 99 | Other Place of Service |
Provider Signature CodeProvider Signature Code
A Y value indicates the provider signature is on file; an N value indicates the provider signature is not on file with the provider.
Signature Generated by ProviderSignature Generated by Provider (check box)
Mark check box if signature generated by provider or an entity other than the patient because the patient was not physically present for services. Required when a signature was executed on the patient’s behalf under state or federal law.
eMEDIX Online | ©copyright 2025 CompuGroup Medical, Inc. All rights reserved.